
next
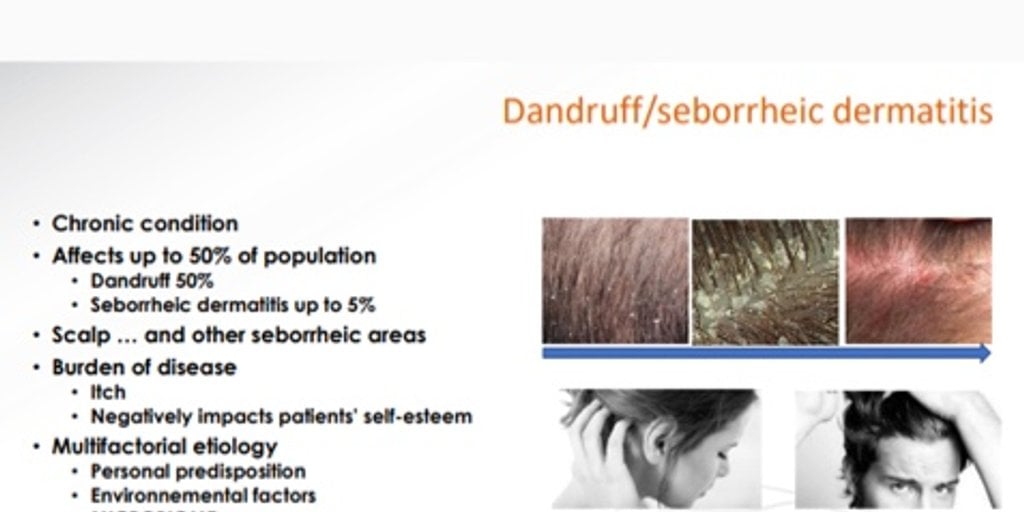
Dandruff/Seborrheic dermatitis


Seborrheic dermatitis (SD) is a chronic and relapsing inflammatory skin condition of sebum-rich areas such as the scalp. It is characterized by erythema, mild- to- moderate scaling resulting in an oil and flaky scalp, and is sometimes associated with pruritus. In the adult population, its prevalence is up to 5%, with a higher prevalence in immunocompromised patients and in patients with neurological condition. When only mild scaling without visible inflammation is observed, SD is called dandruff. The prevalence of dandruff in the general population has been estimated between 15% and 20%. Various environmental, intrinsic and host immune factors may contribute to the development of SD, leading to an alteration of the sebaceous gland activity and sebum composition, epidermal barrier function and skin surface fungal colonization, which ultimately leads to inflammation. Among these factors, lipophilic Malassezia fungi may play a key role.1
1. Massiot P. et al. , Continous improvement of mild-to-moderate seborrheic dermatitis and rebalancing of the scalp microbiome using a selenium disulfide-based shampoo after an initial treatment with ketoconazole, J Cosmet Dermatol. 2021;00:1–11

The central role of microbiome
What is the scalp microbiome?
The microbiome is the invisible ecosystem of living microorganisms which is integral part of the skin’s surface. It’s balance is essential to our skin health. Just like skin microbiome, preserving the balance of the scalp microbiome is a major challenge for the good health of the scalp. When it is altered , scalp issues may occur.
Dercos is pionner of scalp microbiome science, conducting research and clinical studies to explore the role of scalp microbiome in different scalp diseases beyond dandruff and sensitivity.
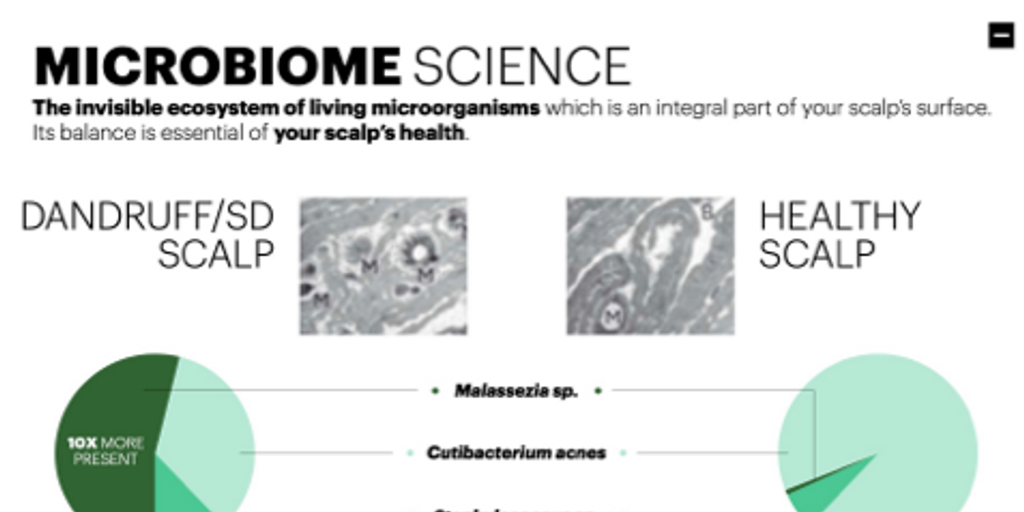

What’s the difference between a non dandruff scalp microbiome and a dandruff scalp microbiome?
Dandruff and SD conditions present an imbalance in the proportion of fungal and bacterial populations in the scalp microbiome:
- Increase in Malassezia sp. (10x more present)
- Decrease of Cutibacterium Acnes.
- Inbalance between Malassezia sp. and Cutibacterium Acnes.
- Increase Malassezia sp. / Cutibacterium Acnes ratio.
- Increase Staphylococcus sp. / Cutibacterium Acnes ratio.

Scalp microbiome and dandruff: the love story
Clinical studies about Dandruff and Seborrheic dermatitis

Selenium disulfide studies
Two single-center studies (one vehicle-controlled and one open-label) to investigate the mode of action of selenium disulfide (SeS2) in a shampoo.
Dercos DS maintenance observational study in Eastern Europe
An international multi-center, observational study of 1,047 subjects to assess the maintenance effect of an ses2-based shampoo in adults with severe dandruff or ssd after an initial medicated treatment.


Patient advice leaflet: dandruff
Which topic are you interested in?


Get free unlimited access to more articles and resources like this!
L'Oréal Dermatological Beauty Pro is a digital community empowering healthcare professionals to improve their daily practice of dermatology through cutting edge research, science and education on skin and hair care.
Sign Up For Free TodayAlready registered? Log in