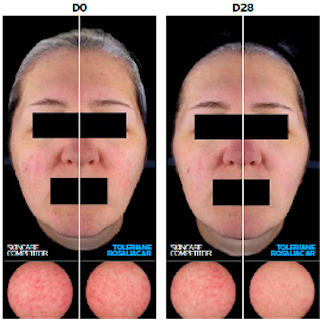
Toleriane Rosaliac AR new proven efficacy on patients with rosacea-prone skin
 May. 2025
May. 2025
Sensitive skin is clinically defined by characteristic sensory perceptions including:

Although sensitive skin was initially believed to be an abnormal reaction to common products and occurred in only small subset of consumers, epidemiological surveys consistently find a high prevalence of sensitive skin across the industrialized world.
The majority of women in the USA, Europe, and Japan (which represents the vast majority of patients queried to this date) now believe that they have sensitive skin.2 Rates of skin sensitivity have increased steadily over time, particularly among men.3
Sensitive skin, although now largely recognized as a genuine phenomenon of physiological origin, is still a subjective complaint with no consistent associations, no likely aetiologies defined, no predictable or classical visible signs of irritation, no immunological verifiable response, and no accepted and reproducible diagnostic test. Although it is clear that specific individuals have heightened sensitivity to different kinds of sensory and physical irritants, observed reactions are not predictive of generalized sensitivity, and the relationship between observed sensitivities is unclear.4
Evidence suggests that sensitive skin may not be a single condition, but one that encompasses different categories of subjects and sensitivities based on different mechanisms – not a single entity, but a heterogeneous phenomenon. Multiple aetiologies would not be farfetched, as the nervous system does not act in isolation but is interdependent with both the immune system and the skin, sharing numerous cellular contacts as well as the same language of cytokines and neurotransmitters. All three interact to affect cutaneous responses.4,5
A majority of sensitive skin sufferers report unpleasant sensory responses to:

Possible contributors to sensititve skin:
Part of the reason for the observed breakdown between sensory effects and objective signs is the fact that an objective sign like erythema is the end result of a complex, multistep physiological process. Numerous underlying processes (e.g. changes in blood flow, moisture content, pH) would be expected to occur before the appearance of visible external changes.8
Methodology is needed, which could increase the ability to predict and quantify these subjective patient responses. Three possible approaches include the following:8
Data continue to accumulate which suggests a link between atopy and sensitive skin.
Sensitive skin is also predominantly sensory in nature and thus ultimately a neurological disorder: sensory differences may be related to innervation. Dermal nerve fibres extend throughout viable epidermis as free nerve endings, but the epidermal component of this network is still poorly characterized. Epidermal nerve density variation could explain the different sensitivity thresholds in various anatomical sites. Hyperreactivity of the neural response of the skin is postulated to play a role. Possible mechanisms for neural system hyperreactivity include nerve fibres; endothelin receptors; burn, itch, and heat receptors; cold receptors; and neutrophins.4
Subclinical irritation may be the key to understanding sensitive skin, as sensations elicited by product exposure are generally discerned long before observable differences. One significant advance in methodology with the potential to greatly increase understanding of sensitive skin is the development of new, non-invasive techniques (like crosspolarized light-enhanced visualization), which has yielded results that show good correlation with sensory perceptions and which provides the ability to measure subclinical damage.4
An immediate need is to build on what is known with improved techniques, carefully crafted protocols that evaluate appropriate exposures and study populations, and rigorous methodological and statistical procedures, bringing the study of sensitive skin out of the realm of fairy tales and into the realm of a genuine physiological disorder worthy of focused research.
The challenge of the future is to unravel the biological link between subjective clinical signs and their physical sequelae as a means to develop appropriate diagnostic criteria as well as to understand the aetiology of this still largely mysterious disorder.4
Bibliography
